Pelvic organ prolapse (POP) is commonly first identified and managed within gynaecology — and in many cases, this is entirely appropriate. Early-stage prolapse, mild symptoms, and conservative management often fall well within standard gynaecological care. However, not all prolapse is the same. As prolapse becomes more advanced, recurrent, or functionally disruptive, it can evolve into […]

Pelvic organ prolapse (POP) is commonly first identified and managed within gynaecology — and in many cases, this is entirely appropriate. Early-stage prolapse, mild symptoms, and conservative management often fall well within standard gynaecological care.
However, not all prolapse is the same.
As prolapse becomes more advanced, recurrent, or functionally disruptive, it can evolve into a far more complex condition — one that extends beyond gynaecology alone and into the realm of specialised urological and pelvic reconstructive surgery.
Understanding when this transition occurs is critical for both patients and referring clinicians.
Understanding Pelvic Organ Prolapse Beyond the Basics
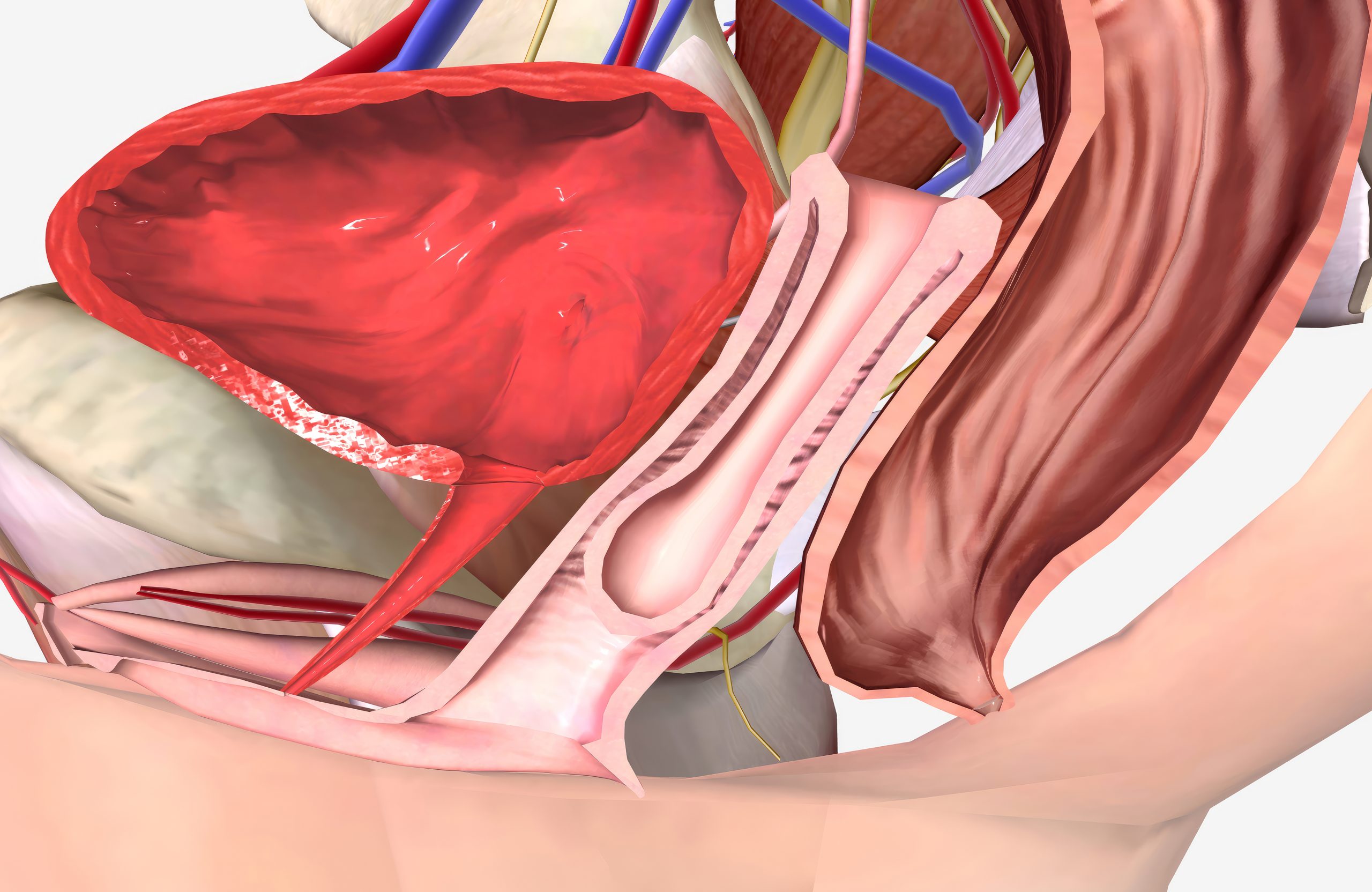
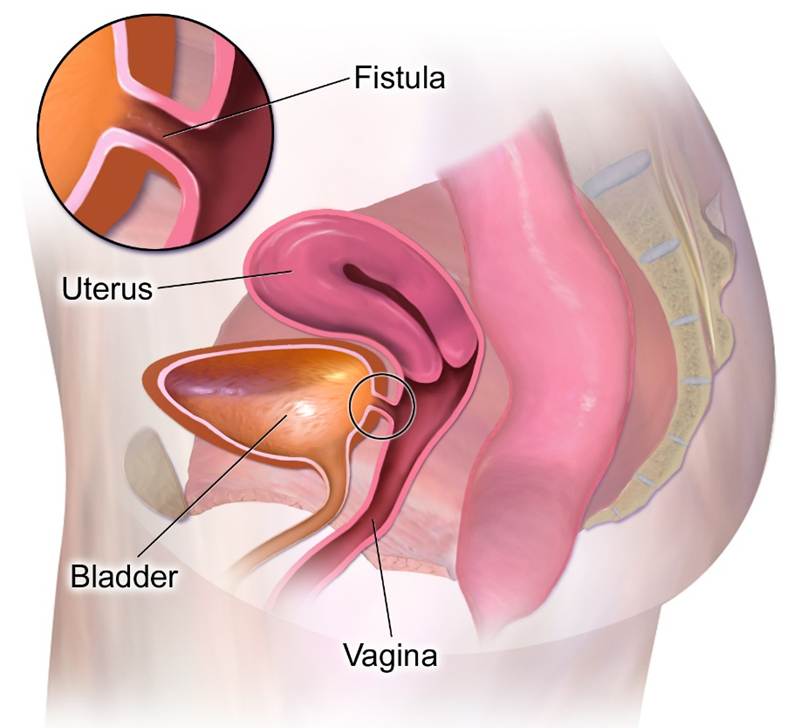
Pelvic organ prolapse occurs when one or more pelvic organs descend from their normal position due to weakening of the pelvic floor support structures. These organs may include:
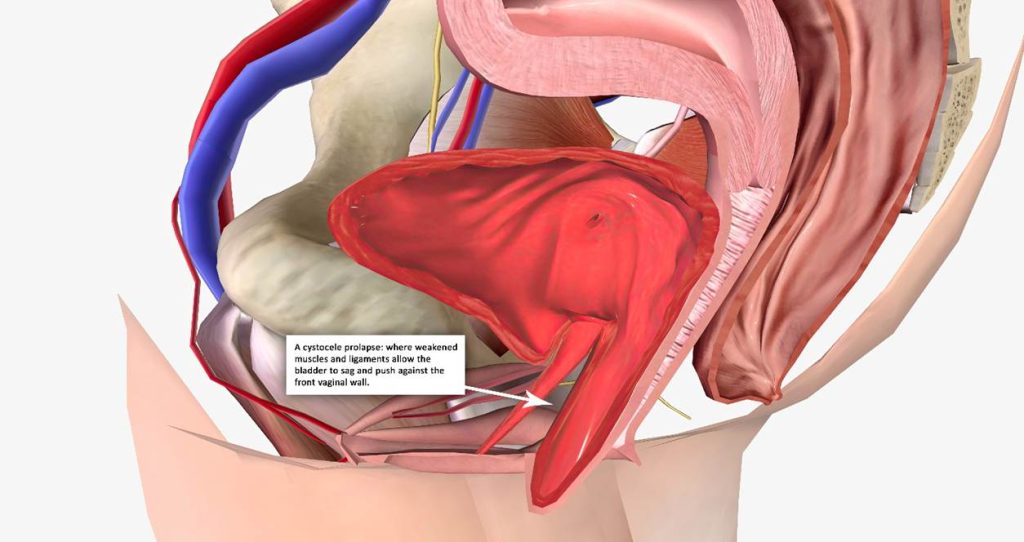
(A cystocele prolapse: where weakened muscles and ligaments allow the
bladder to sag and push against the front vaginal wall.)
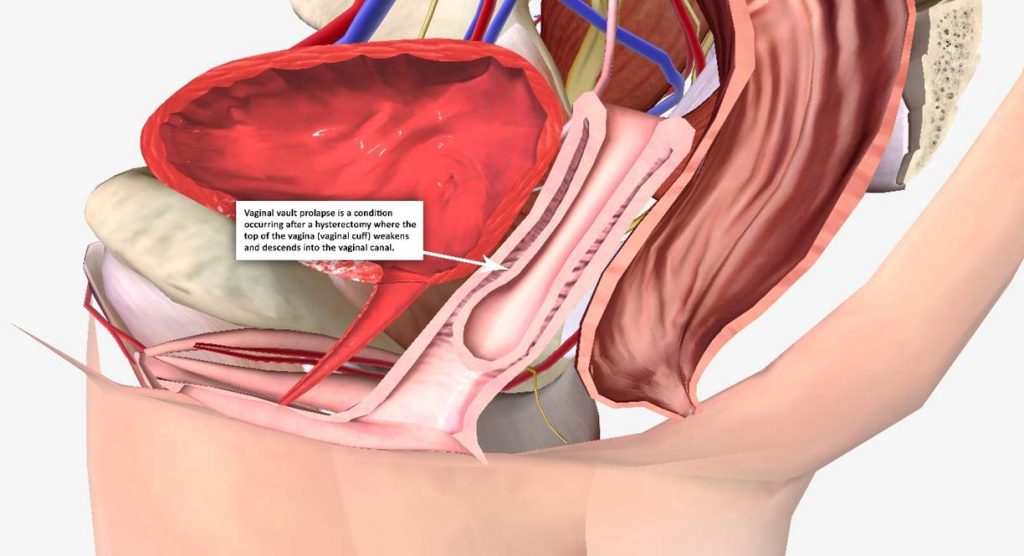
(Vaginal vault prolapse: a condition occurring after a hysterectomy where the top
of the vagina (vaginal cuff) weakens and descends into the vaginal canal.)
While these organs are often discussed individually, the pelvic floor does not function in isolation. It is a highly integrated system consisting of muscles, ligaments, connective tissue, fascia, and neural control mechanisms. When one component fails, the entire system is affected.
This is why treating prolapse as a single-organ problem can sometimes lead to incomplete correction or recurrence.
When Prolapse Becomes a Surgical Reconstruction Problem
There is a point at which pelvic organ prolapse is no longer simply about support or symptom relief — it becomes a reconstructive challenge.
This is often the case when patients experience:

At this stage, the goal is no longer just to reposition organs, but to restore anatomy, protect function, and ensure long-term durability.
The Urogynaecological Perspective: Where Urology Enters the Picture
Many prolapse cases involve the bladder, urethra, and surrounding support structures — placing them firmly within urological territory.
Advanced prolapse frequently affects:
If these structures are not properly addressed during prolapse surgery, patients may experience persistent or new urinary symptoms after surgery — including incontinence, obstruction, or incomplete bladder emptying.
This is where urogynaecological expertise becomes essential. Surgical planning must protect urinary function while correcting pelvic support failure.
Why Advanced Prolapse Requires Specialist Surgical Expertise
Complex prolapse surgery demands a detailed understanding of:
Overcorrection can be just as problematic as undercorrection. Inadequate reconstruction increases the risk of recurrence, while excessive tension may compromise function or cause pain.
Specialist surgeons focus not on “doing more surgery,” but on doing precise, anatomical reconstruction that lasts — often using minimally invasive techniques that reduce recovery time and surgical trauma.

(Sacrocolpopexy restores normal pelvic anatomy by lifting the vagina back into its natural
position and anchoring the front and back vaginal walls to the strong ligament at the sacral
promontory for durable support.)
The Role of Biomechanics in Prolapse Surgery
Pelvic organ prolapse is fundamentally a biomechanical failure.
Successful surgical repair depends on restoring balance — not just anatomy. This includes:
Dr MC Conradie’s background in biomechanics brings a unique dimension to prolapse surgery. This expertise directly informs surgical technique, planning, and outcomes — and has led to the design and commissioning of specialised medical equipment used in prolapse surgical procedures.
This biomechanical approach aims to facilitate in the understanding of the anatomy and surgical dissection of the pelvic organs. This will ultimately translate to improved surgical success and form results.
When to Refer: Guidance for Patients and Clinicians
Patients should consider specialist care if they:
Referring clinicians should consider specialist referral when:
Early referral can prevent repeated procedures and protect long-term pelvic health.
Specialist Care for Complex Pelvic Organ Prolapse
Dr MC Conradie is a urology specialist with a dedicated focus on complex urogynaecological and pelvic reconstructive surgery. Her practice centres on minimally invasive techniques, advanced anatomical reconstruction, and long-term functional outcomes.
Her expertise spans both patient care and surgical innovation — ensuring that each procedure is guided by precision, biomechanics, and evidence-based practice.
Redefining Prolapse Care
Pelvic organ prolapse is not always a gynaecology issue.
In complex, recurrent, or advanced cases, it becomes a condition that requires specialist urological and reconstructive surgical care. Recognising this transition is essential — because the right intervention, at the right time, can make the difference between repeated symptoms and lasting recovery. If prolapse is affecting quality of life or has become difficult to manage, specialised care matters.